
Contrast Media
Mindy M. Horrow, MD, FACR
Director of Body Imaging
Albert Einstein Medical Center

Must one obtain informed consentbefore a contrast injection?
•A. Yes
•B. No
Must one obtain informed consentbefore a contrast injection?
•A. Yes
•B. No
Many radiologists, probably a majority,do not obtain informed consent.Instead, it is quite common to use aninformation sheet, as a method toobtain history from the patient andexplain potential risks to the patient.Compared to other procedures in whichwe obtain consent (surgery,angiography, etc.) the risks of contrastare extremely low. Risk of death < 1 in130,000. Risk of renal failure and strokeare also very low.
Millions of radiologic exams are conductedeach year with intravascular contrast.What percentage of studies with non-ioniccontrast have adverse side effects?
•A. 1 – 3
•B. 5 – 12
•C. 12 – 15
•D. 15 – 20
Millions of radiologic exams are conductedeach year with intravascular contrast.What percentage of studies with non-ioniccontrast have adverse side effects?
•A. 1 – 3
•B. 5 – 12
•C. 12 – 15
•D. 15 – 20
Side effects are somewhat higher with ionic contrast.
Which of the following are truestatements about adverse reactions tointravascular contrast?
•A. Virtually all life threatening events occurimmediately after the injection.
•B. A test injection is not helpful to decrease theincidence of severe reactions.
•C. Adverse reactions are higher with intravenouscompared to intra-arterial injections.
•D. Most adverse side effects are life threatening.
Which of the following are truestatements about adverse reactions tointravascular contrast?
•A. Virtually all life threatening events occurimmediately after the injection.
•B. A test injection is not helpful to decrease theincidence of severe reactions.
•C. Adverse reactions are higher with intravenouscompared to intra-arterial injections.
•D. Most adverse side effects are life threatening.
•Life threatening reactions may occurimmediately or within 20 minutes of theinjection and may start with a mildreaction.
•In the past, it was believed that intra-venous injections were associated withgreater numbers of adverse reactions.Data now shows that they are more likelywith the intra-arterial route.
Which of the following isassociated with an increased riskof contrast reactions?
•A. Hayfever
•B. Shellfish allergy
•C. Asthma
•D. Diabetes
Which of the following isassociated with an increased riskof contrast reactions?
•A. Hayfever
•B. Shellfish allergy
•C. Asthma
•D. Diabetes
•History of multiple, severe allergies,including asthma, does increase risk ofcontrast reaction, but only by very smallpercentage. Most such reactions will beminor.
•Asthma increases risk of bronchospasmonly.
•Shellfish allergy is NOT a predictor ofcontrast allergy. Organic iodide foundin shellfish is an essential element sopeople CANNOT be allergic to it.
•Diabetes is not a risk factor for adversereactions. Other specific conditionswhich are risk factors include:pheochromocytoma, thyrotoxicosis,dysproteinemias (multiple myeloma) andsickle cell disease.
If a patient has had a prior “allergic”reaction to iodinated contrast,
•A. They should never receive anotherinjection of iodinated contrast.
•B. Adverse reactions to contrastresemble allergic reactions, but areNOT true allergies.
•C. It is likely they will have anotherreaction if they receive contrast again.
•D. They should not receive gadoliniumcontrast agents for MRI.
If a patient has had a prior “allergic”reaction to iodinated contrast,
•A. They should never receive anotherinjection of iodinated contrast.
•B. Adverse reactions to contrastresemble allergic reactions, but areNOT true allergies.
•C. It is likely they will have anotherreaction if they receive contrast again.
•D. They should not receive gadoliniumcontrast agents for MRI.
•Contrast agents are small molecules,probably too small to act as antigens.
•No antibodies to contrast agents havebeen identified in patients with systemic“allergic” type reactions.
•Patients with adverse reactions tocontrast are unlikely to have a similar ormore severe event if injected again.Likelihood of recurrence is 8% to 25%.
Does pretreatment with corticosteroidsprevent recurrent contrast reactions?
•A. Always
•B. Sometimes
•C. Never
Does pretreatment with corticosteroidsprevent recurrent contrast reactions?
•A. Always
•B. Sometimes
•C. Never
•Pretreatment only effective in preventingminor reactions.
•Unlikely to prevent life-threateningreactions.
•Steroid use must begin at least 12 hoursbefore injection to prevent even minorreactions.
•Use of a contrast agent patient has notbeen exposed to previously may help,but one must always be ready to treat lifethreatening reactions.
Which of the following statementsregarding vaso-vagal reactions is false?
•A. They are relatively common reactions inpeople with increased vagal tone.
•B. Effects include decrease SA and AV nodalactivity, inhibition of AV conduction andperipheral vasodilatation.
•C. The reactions are characterized byhypertension and tachycardia.
•D. The reactions are related to anxiety and mayoccur with placement of the IV or discussion ofthe procedure.
Which of the following statementsregarding vaso-vagal reactions is false?
•A. They are relatively common reactions inpeople with increased vagal tone.
•B. Effects include decrease SA and AV nodalactivity, inhibition of AV conduction andperipheral vasodilatation.
•C. The reactions are characterized byhypertension and tachycardia.
•D. The reactions are related to anxiety and mayoccur with placement of the IV or discussion ofthe procedure.
The hallmark is hypotension and bradycardia
Mild contrast reactions include all ofthe following except:
•A. Dizziness
•B. Itching
•C. Sweats
•D. Nasal stuffiness
•E. Swelling of eyes, face
•F. Anxiety
•G. Hypotension
Mild contrast reactions include all ofthe following except:
•A. Dizziness
•B. Itching
•C. Sweats
•D. Nasal stuffiness
•E. Swelling of eyes, face
•F. Anxiety
•G. Hypotension
Requires observation, reassurance, but usually no treatment
Moderate contrast reactions include allof the following except:
•A. Mild laryngeal edema
•B. Hypertension or hypotension
•C. Bronchospasm
•D. Cough
•E. Dyspnea
•F. Tachycardia / bradycardia
Moderate contrast reactions include allof the following except:
•A. Mild laryngeal edema
•B. Hypertension or hypotension
•C. Bronchospasm
•D. Cough
•E. Dyspnea
•F. Tachycardia / bradycardia
Treatment typically required as well as observation forprogression to severe reactions.
Severe contrast reactions include all ofthe following except:
•A. Moderate and severe laryngeal edema
•B. Seizures
•C. Unresponsiveness
•D. Cardiopulmonary arrest
•E. Symptomatic urticaria
Severe contrast reactions include all ofthe following except:
•A. Moderate and severe laryngeal edema
•B. Seizures
•C. Unresponsiveness
•D. Cardiopulmonary arrest
•E. Symptomatic urticaria
Requires prompt treatment including hospitalization
Which of the following is important inassessing a patient’s risk to contrast?
•A. History of renal dysfunction
•B. History of diabetes
•C. Patients with angina or CHF with minimalexertion
•D. Patients with primary pulmonary HTN,severe cardiomyopathy or severe aorticstenosis
•E. All of the above
Which of the following is important inassessing a patient’s risk to contrast?
•A. History of renal dysfunction
•B. History of diabetes
•C. Patients with angina or CHF with minimalexertion
•D. Patients with primary pulmonary HTN,severe cardiomyopathy or severe aorticstenosis
•E. All of the above
Which of the following is true regardingpremedication - contrast strategies inpatients with prior reactions?
•A. Use HOCM
•B. Use a combination of steroids andantihistamines
•C. Intravenous administration ispreferable to oral
•D. In emergency situations, do not useintravenous contrast if there is a historyof allergic type reactions.
Which of the following is true regardingpremedication - contrast strategies inpatients with prior reactions?
•A. Use HOCM
•B. Use a combination of steroids andantihistamines
•C. Intravenous administration ispreferable to oral
•D. In emergency situations, do not useintravenous contrast if there is a historyof allergic type reactions.
•Oral administration is preferable tointravenous
•In emergency situations, use IVcorticosteroid every 4 hours plus anH-1 antihistamine 1 hour beforeprocedure.
Regarding contrast nephrotoxicity:
•Defined as a sudden change in renal statusafter contrast administration without othercauses.
•Exact pathophysiology is due to osmotic andchemotoxic effects and is not wellunderstood.
•Major risk factor is underlying renaldysfunction. Never occurs in patients withtruly normal baseline renal function.
Regarding contrast nephrotoxicity:
•Diabetes, probably not an independent riskfactor, but IS a major contributing factor inpresence of renal dysfunction.
•Additional concerns: dehydration, poor renalperfusion as in CHF, nephrotoxic drugs.
•Increased volume of contrast will increaselikelihood of contrast nephropathy, only ifpatient has underlying renal dysfunction.
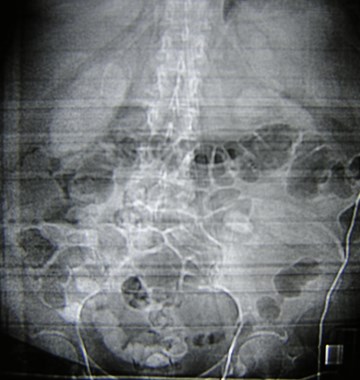

1 day after cardiac catheterization
Hemoglobin
Contrast induced nephropathy
Vicarious excretion in bile

Cardiac catheterization several days earlier
Creatinine increased further
CT: no contrast given
Recommendations for prevention ofcontrast induced renal failure includeall of the following except:
•A. Hydration
•B. Mannitol and/or furosimide
•C. Oral acetylcysteine (Mucomist)
•D. Increased interval between contrastmedia exams
•E. Decreased contrast dose.
Recommendations for prevention ofcontrast induced renal failure includeall of the following except:
•A. Hydration
•B. Mannitol and/or furosimide
•C. Oral acetylcysteine (Mucomist)
•D. Increased interval between contrastmedia exams
•E. Decreased contrast dose.
•Recommended dose of acetyl cysteine:600 mg BID, the day before and day ofcontrast injection.
•Hydration with 5% D/W with 3 ampsNaHCO, 200 ml for 1 hour before and75 ml/hr for 6 hours after theprocedure.*
•Mannitol has no effect and furosemidemay exacerbate the renal dysfunction.
*Recommendation of AEMCsection of Nephrology
Indications for measurement of serumcreatinine before contrastadministration include all except:
•A. History of kidney disease, including renal tx
•B. Family history of renal failure
•C. Insulin dependent diabetes
•D. All patients
•E. Multiple myeloma
•F. Regular use of nephrotoxic antibiotics such asaminoglycosides.
Indications for measurement of serumcreatinine before contrastadministration include all except:
•A. History of kidney disease, including renal tx
•B. Family history of renal failure
•C. Insulin dependent diabetes
•D. All patients
•E. Multiple myeloma
•F. Regular use of nephrotoxic antibiotics such asaminoglycosides.
Patients without these factors do NOT requiremeasurement of creatinine before contrast.
Patients on dialysis
•A. Must never receive intravenouscontrast
•B. Require emergent dialysis aftercontrast studies
•C. Require dialysis within 24 hours.
•D. None of the above
Patients on dialysis
•A. Must never receive intravenouscontrast
•B. Require emergent dialysis aftercontrast studies
•C. Require dialysis within 24 hours.
•D. None of the above
Patients on chronic dialysis may receive intravenouscontrast and have their dialysis at the regular, scheduledtime. Patients on dialysis emergently or intermittently areat very great risk for nephrotoxicity and alternative imagingstudies are preferred.
Regarding metformin therapyand intravenous contrast:
•A. Metformin should be withheld for 48hours after contrast administration andre-instated only after normal renalfunction is established.
•B. Metformin should be withheld for 24hours before contrast administration.
•C. Metformin should be withheld beforestudies with gadolinium.
Regarding metformin therapyand intravenous contrast:
•A. Metformin should be withheld for 48hours after contrast administration andre-instated only after normal renalfunction is established.
•B. Metformin should be withheld for 24hours before contrast administration.
•C. Metformin should be withheld beforestudies with gadolinium.
•Elevated levels of Metformin increase risk of lacticacidosis, which may be fatal in up to 50% of cases.
•Metformin is excreted by the kidneys, and thuscontraindicated in patients with renal dysfunction.
•Hypothesis that Metformin and iodinated contrastwill lead to an increased risk of lactic acidosis, hasbeen disproved.
•Package insert is still cautious, recommending thatMetformin be stopped for 48 hours after iodinatedcontrast.
Medications containing Metformin include: Avandamet,Glucophage, Glucophage XR, Glucovance, Metaglip
If extravasation of contrast materialoccurs:
•A. The patient will complain of pain during theinjection.
•B. Only occurs with power injections
•C. Most patients recover without sequlae thoughoccasional, severe injuries can occur, includingulceration and tissue necrosis, compartmentsyndrome chronic fibrosis and muscle atrophy.
If extravasation of contrast materialoccurs:
•A. The patient will complain of pain during theinjection.
•B. Only occurs with power injections
•C. Most patients recover without sequlae thoughoccasional, severe injuries can occur, includingulceration and tissue necrosis, compartmentsyndrome chronic fibrosis and muscle atrophy.
Some patients may NOT complain of any pain whenextravasation occurs. Extravasation may occur withhand or power injections.
If extravasation occurs, one should
•Elevate the affected extremity.
•Apply warm compresses.
•Apply cold compresses.
•Consider a surgical consultation.
•Outpatients should be released only after initialsigns and symptoms have improved and nofurther symptoms have occurred.
•Notify the referring physician
•Document the occurrence in the medical record.
There is no consensus regarding the treatment ofcontrast extravasation.
Regarding air embolisation all of thefollowing are true except:
•A. This is a fatal complication
•B. Diagnosed on CT as air bubbles or air fluidlevels in veins, pulmonary artery or rightventricle.
•C. Large amounts may result in dyspnea, cough,chest pain, pulmonary edema, tachycardia,hypotension or wheezing.
•D. Treatment includes 100% O and placingpatient in left lateral decubitus position.
Regarding air embolisation all of thefollowing are true except:
•A. This is a fatalcomplication
•B. Diagnosed on CT as airbubbles or air fluid levelsin veins, pulmonary arteryor right ventricle.
•C. Large amounts mayresult in dyspnea, cough,chest pain, pulmonaryedema, tachycardia,hypotension or wheezing.
•D. Treatment includes100% O and placingpatient in left lateraldecubitus position.
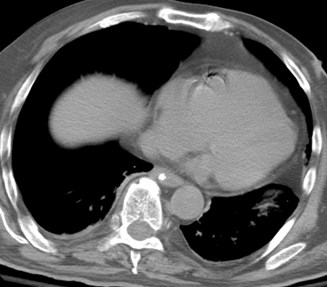
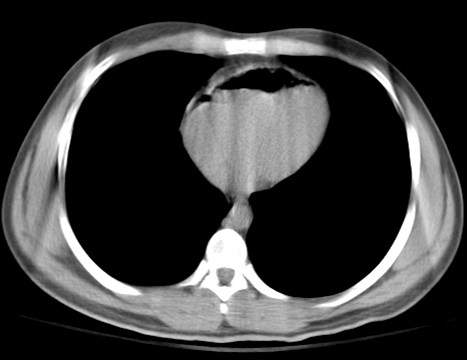
ER CT, prior to IV contrast
Mothers who are breast feeding andneed to receive intravenous contrastshould:
•A. Cease breast feeding
•B. Continue breast feeding immediately
•C. Wait 24 hours before re-starting breast feeding
Mothers who are breast feeding andneed to receive intravenous contrastshould:
•A. Cease breast feeding
•B. Continue breast feeding immediately
•C. Wait 24 hours before re-starting breast feeding
•Plasma half life of IV contrast is approximately 2hours with nearly 100% cleared from bloodstreamin 24 hours.
•< 1% is excreted into breast milk in first 24 hoursand < 1% of ingested contrast is absorbed from itsGI tract, the expected dose absorbed by infantfrom breast milk is < 0.01 % of IV dose given tomother.
•Thus, ACR believes it is safe for mother andinfant to continue breast feeding after IV contrast.
•If mother remains concerned, she may abstainfrom breast feeding for 24 hours.
Regarding the use of contrast inpregnant patients:
•A. Contrast does not cross the placenta
•B. Teratogenic effects of contrast medium arewell documented in the literature.
•C. Sufficient evidence available to conclude thatcontrast agents pose no risk.
•D. Recommended that pregnant patientsundergoing imaging with ionizing radiation andiodinated contrast provide informed consent todocument that they understand the risk/benefitsof the procedure.
Regarding the use of contrast inpregnant patients:
•A. Contrast does not cross the placenta
•B. Teratogenic effects of contrast medium arewell documented in the literature.
•C. Sufficient evidence available to conclude thatcontrast agents pose no risk.
•D. Recommended that pregnant patientsundergoing imaging with ionizing radiation andiodinated contrast provide informed consent todocument that they understand the risk/benefitsof the procedure.
Management of Urticaria
•Discontinue injection if not completed
•No tx in most cases
•If tx necessary, benadryl PO/IM/IV 25 – 50 mg
•If severe or widely disseminated, epinephrine SC(1 : 1000), 0.1 – 0.3 ml
Management of Facial orLaryngeal Edema
•Epinephrine SC or IM (1 : 1000) 0.1 – 0.3 ml
•If hypotension evident, epinephrine (1 : 10,000)slowly IV 1 ml = 0.1 mg. Repeat as needed to 1mg.
•O via mask 6 – 10 liters/min
•If severe edema, or unresponsive to therapy, callfor help
Management of Bronchospasm
•Mask O, 6 – 10 liters/min
•Monitor ECG, pulse oximeter, blood pressure
•Give beta-agonist inhalers
•Epinephrine SC or IM (1 : 1,000), 0.1 – 0.3 ml or ifhypotension, IV ( 1 : 10,000) slowly up to 1 mg
•Call for assistance for severe bronchospasm orhypoxemia
Hypotension with Tachycardia
•Elevate legs
•Monitor ECG, pulse oximeter, bloodpressure
•Give mask O
•Rapid IV fluids
•If poorly responsive, IV epinephrine
Hypotension with Bradycardia(vagal reaction)
•Monitor vital signs
•Elevate legs
•Secure airway, mask O
•Secure IV access, give fluids
•Atropine 0.6 – 1 mg IV slowly if patient does notrespond to other measures
•Ensure complete resolution of symptoms prior todischarge

References:
1.ACR Manual onContrast Media, Version5.0
2.2. Bettmann, MAFrequently AskedQuestions: IodinatedContrast Agents.Radiographics 2004;24:S3-S10